SIGN 160 Lecture: Lesson 3
- The Ear and Etiology of Hearing Loss
1. How we hear
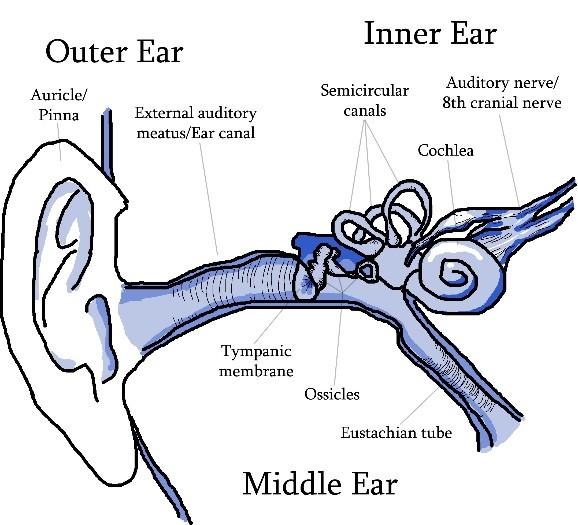
Hearing starts at the outer ear (pinna or auricle) when the sound is channeled down the ear canal (external auditory meatus) to the first part of the middle ear – the eardrum (tympanic membrane). Sound causes the ear drum to vibrate and sets in motion a chain of vibrations transmitted sequentially by three small bones (ossicles) called the hammer (malleus), anvil (incus) and the stirrup (stapes).
(See diagram Below)
Outer Ear – The passage for wave/sound energy to enter the ear
- Auricle/Pinna
- Ear Canal/external auditory meatus
Middle Ear – Changes wave/sound energy to mechanical energy; conducts sound from our to inner ear
- Ear drum/Tympanic membrane
- Ossicles: Hammer/Malleus, Anvil/Incus, Stirrup/Stapes
- Eustachian tube
Inner Ear – Changes mechanical energy to electrical energy/nerve pulses; prepares information to be send to the brain
- Cochlea, including hair cells
- Semicircular canals
- Auditory nerve/VIII Cranial nerve
Auditory Cortex – The areas of the brain where electrical energy/nerve pulses are interpreted and meaning is assigned
- Temporal lobe
(please refer to picture of ear)
2. Terminology and types of hearing loss
pre-lingual deafness: deafness is present before language is acquired
post-lingual deafness: deafness occuring following the development of language (and speech)
Adventitious deafness: deafness occurred after birth
Congenital deafness: deafness present since birth
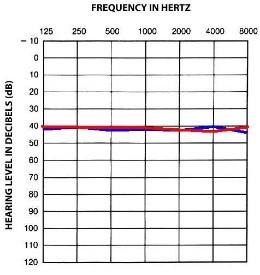
Conductive hearing loss – the outer and/or middle ear is not able to conduct sound energy to the inner ear. This type of loss can be temporary and corrected by medical treatment. Examples of conductive loss are wax buildup, ear infection, fusion of the ossicles. (often results in a “flat” audiogram)
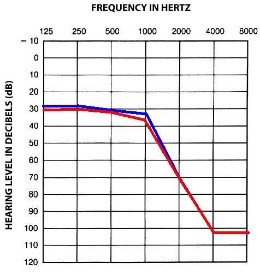
Sensorineural hearing loss – caused by the damage of the hair cells or nerve cells in the inner ear. This tends to be permanent. This type of loss can be caused by environmental factors such as noise, toxic medications and head injury. Sensorineural hearing loss can be genetic and progressive. (often results in a “sloping” audiogram)
Mixed hearing loss – A combination of both types (conductive and sensorineural) of hearing losses
A syndromic loss indicates a genetic syndrome that carries other medical or physical symptoms along with hearing loss.
A nonsyndromic loss indicates hearing loss alone.
3. Causes of Hearing Loss
Nongenetic Causes
Infections/Virus: Some infections or viruses can cause deafness, such as:
- Rubella (or German measles) – harmful if pregnant mother infected; last major outbreak 1964-1965 (12,000 born), if exposed 60%-80% chance infant will have hearing loss. Epidemic during 1964-1965 during which time 12,000 infants were born with hearing loss.
- Cytomegalovirus (CMV) – harmful if pregnant mother exposed; type of herpes; symptoms of CMV in children include mental retardation, behavioral problems, neurological problems, cerebral palsy, learning disabilities, hearing loss, etc. Hearing loss appears in 30%-60% of infants born with CMV. Also, late onset hearing loss is possible so children should have ongoing hearing evaluations.
- Herpes and HIV – Infants born exposed to the herpes simplex virus and HIV are at risk for hearing loss among other problems
- Meningitis – infection of the membranes surrounding the brain; bacterial form is leading cause of deafness; negative affects are seen more in younger children because they cannot verbalize symptoms (headache, stiff neck). If gets to this advanced stage the likelihood of hearing loss is 40%. Other long term affects can be aphasia (language problems), behavioral problems, and balance problems.
- Congenital Toxoplasmosis – parasitical infection caused by exposure to cat liter, feces and soil/dirt. Affects pregnant women during gestational period. Around 15-26% of children experience hearing loss.
Erthroblastosis Fetalis – (also called Rh Factor) – caused by blood incompatibility between mother and fetus. Currently Rh factor immunizations for the mother and blood transfusions for the infant after birth can prevent symptoms. More than 70% of children with Rh factor may present additional disabilities such as cerebral palsy, coordination problems and language difficulties
Ototoxic Drugs – medicines that cause hearing loss. Often given to save the life of the individual (antidepressants, chemotherapy drugs), sometimes not (aspirin). Sometimes it is not known if the hearing loss is caused by the disease or the drug used to treat the disease.
Prematurity – 10% of premature babies will have a sensorineural hearing loss. Prematurity does not cause deafness, but is linked with it.
Genetic Causes
Genetic transmission of deafness includes three kinds of genetic transmission:
- Autosomal dominant or autosomal recessive inheritance
- X linked recessive inheritance
- Mitochondrial inheritance (from the mother)
Major Genetic syndromes involving deafness include:
- Brachial Oto Renal Syndrome (BOR)
- Autosomal dominant, this occurs in 2% of Deaf adults. This is the most common genetic cause of deafness. Malformed ears, skin tags, and kidney problems. Conductive, sensorineural or mixed loss.
- Jervell and Lange-Nielson Syndrome
- Autosomal recessive. Profound hearing loss with heart problems and fainting.
- Neurofibromatosis Type 2 (NF2)
- Autosomal dominant. Tumors cause progressive hearing loss, dizziness, tinnitus, loss of balance
- Pendred Syndrome
- Autosomal recessive. Sensorineural hearing loss and iodine metabolism problems that can lead to goiter and thyroid problems
- Stickler Syndrome (SS)
- Autosomal dominant. Flattening of the facial profile, cleft palate, vision problems, progressive musculoskeletal problems and hearing loss.
- Treacher-Collins Syndrome
- Autosomal dominant, also called mandibulofacial dystosis or Frenschetti-Klein syndrome, malformations of the external ear, eyes, cheekbones. Conductive hearing loss.
- Usher’s Syndrome
- Autosomal recessive. More than half of all DeafBlind adults. Three types of US, symptoms vary with each type. Usually cause a progressive vision loss.
- Waardenberg Syndrome
- Autosomal dominant. Sensorineural hearing loss. Wide set eyes, a white forelock of hair, skin depigmentation, and two different color eyes are some symptoms but they do not all occur in the same person.
4. Role of an Audiologist
- Testing Hearing
- Determining appropriate amplification
- Rehabilitation
- For adults – instruction on use of amplification systems, strategies for communicating, referral to therapy as needed
- An audiologist will determine whether you have a hearing loss or not, but a medical doctor, ENT (Ear, Nose and Throat doctor) helps to determine cause and surgical/medical treatments
5. Diagnosis of a hearing loss
- Infant hearing screening – almost 100% of hospitals in Michigan are doing these. The Newborn Infant Hearing Screening and Intervention Act of 1999 helps to fund state screening programs. The US average age of identification is 12-36 months.
- In cases where he screenings are not done, parents may notice that the baby is not making developmentally appropriate sounds
- The parents may later notice that the child is note responding to sounds or that they make “mistakes” with language
- Age of Identification seems to be linked to severity of loss – the more mild the loss, the later it is usually found
- Parents may suspect a hearing loss, but cannot convince their medical doctor to make a referral to an audiologist
6. How families deal with the diagnosis of hearing loss
- Devastation, shattered dreams
- Overwhelmed by information and choices
- Grieving – an ongoing process(guilt, anger, depression, anxiety, fear, denial, acceptance)
- Deaf parents will react differently
- Most deaf children (90%) are born to hearing parents
7. Variables that influence how a parent responds to having a child with a hearing loss
- parental responsibilities
- quality/stability of the marriage
- argue – many marriages end in divorce
- parents relationships with their own parents
- birth order of the child with the hearing loss
- their own understanding of hearing loss/deafness – most have no knowledge or experience with deafness
8. Parents tend to fall into one of the following categories
- those who are overprotective
- those who deny the hearing loss
- those who reject the child – react with indifference
- those who seek a cure – wishful thinking
- those who accept their child and the hearing loss
9. Attachment, Development
- Mother/infant relationship can be impacted
- Psychosocial and language development are impacted
10. Services and Resources
- when a child is diagnosed, the parents are given lots of resources on various aspects of hearing loss
- early intervention (birth to three years) law mandates services, in Michigan, Early On provides these services
- they are referred to professionals for treatment for the child
- sometimes the parent’s needs are overlooked
- need to get in touch with their feelings and share them; meet other parents with children who have a hearing loss
-need assistance to see the strengths and weaknesses of their child
-need information on communication and education options
11. Other Family Members
- Siblings – parental attitudes will shape the attitudes of the hearing siblings
- Extended family – it is important to educate people outside of the immediate family; grandparents, aunts, uncles, cousins to reduce anxiety and insure acceptance
- CODAs – Children of Deaf Adults; hearing children of deaf parents have a much different experience growing up that hearing children of hearing parents *Please note that CODAs will be discussed more in detail in Lesson 6*
Conductive Hearing Loss
Sensorineural Hearing Loss